Our process of validating and shortlisting a myriad of clinical needs for a better healthcare service provision.
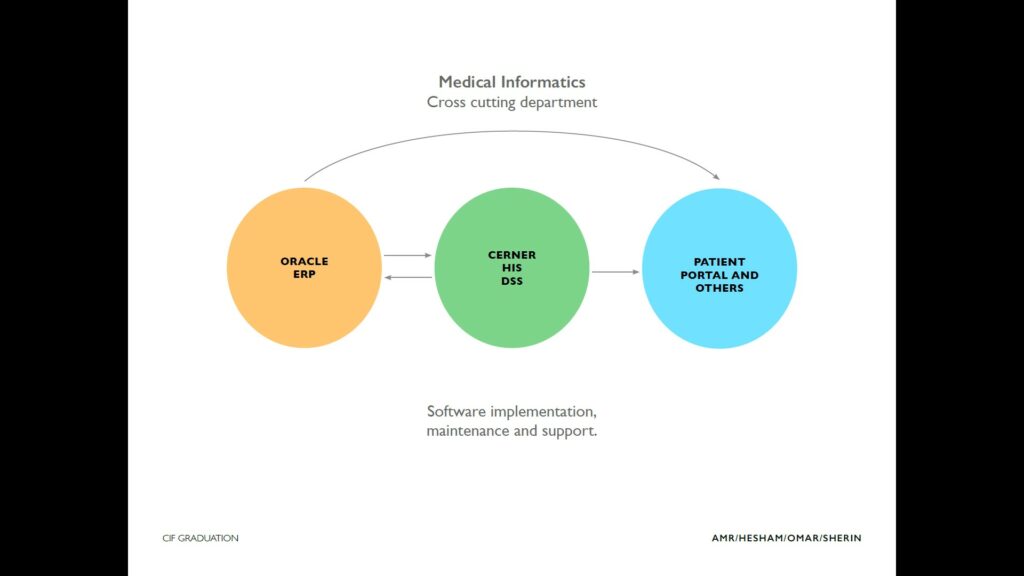
After having an intensive one-week workshop to understand the Stanford Biodesign methodology and how to implement it, we started our Clinical Immersion experience, which took six weeks in the Medical Informatics department at 57357 Hospital. It is a cross-cutting department, responsible for the implementation, maintenance, and support of the health informatics system (HIS), Enterprise resource planning (ERP), Patient portals, and other homegrown software that serves patients and other stakeholders.
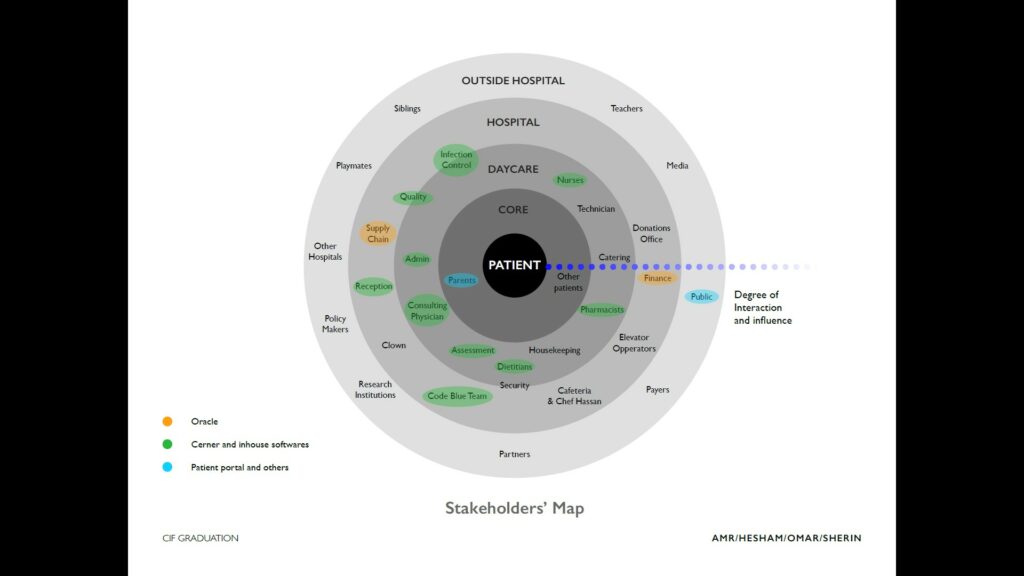
We were lucky to be immersed in this department; it serves nearly every stakeholder in the hospital which enabled us to go everywhere inside the hospital and talk with everyone to hear more about their needs, pain, and thoughts.
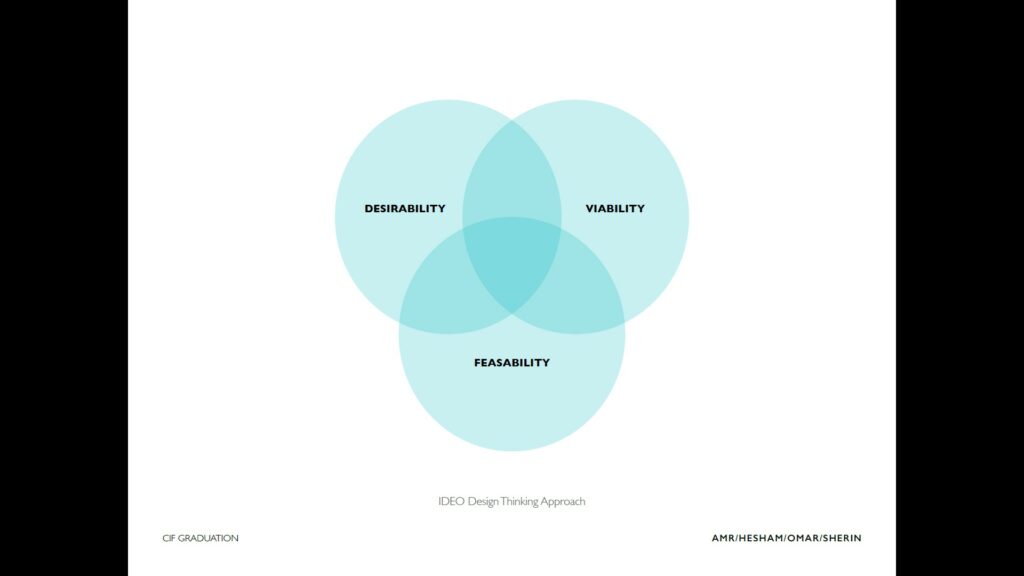
We gathered a lot of observations and needs – to be precise: 985 observations and 234 Needs. Then, we faced a new challenge: We had tons of Data, but we needed to know which of them is desirable, viable, and feasible.
So, it was time to move to a more critical and analytical mindset. We went through a complicated process that was guided with the Biodesign process and we were able to build around it our own tactics to identify the valuable needs, which was a blend of qualitative and quantitative measures.
Working in a multidisciplinary team had a great impact; there was always someone that either has the answer or at least has the basic knowledge that he can with some research build on to find the answer from his perspective. To make use of that and assure that each one of the team gives his opinion about each need, by the end of each stage the ranking was a collective process, each member makes a quick pitch for the needs assigned to him and advocate for his ranking and afterward the rest of the team start building their own ranking.
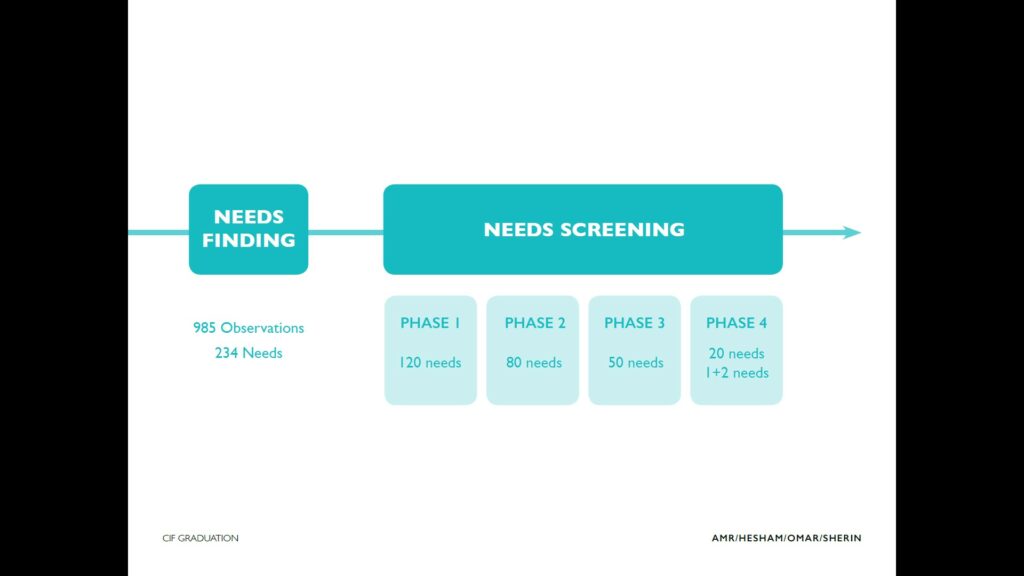
Our need screening process was divided into 4 stages:
First stage
Our goal was to go from 234 to 120 needs we did so by applying the following.
- eliminating replications
- merging the needs that can fit together.
- and rewriting the needs to make sure they are clear and to the point.
Second Stage
To go from 120 to 80 needs we started by doing a quick high-level research on each one of them to build basic perception and start grading and ranking them according to their feasibility, desirability, and viability.
Third Stage
To go from 80 to 50 needs – the time for digging deeper by doing more in-depth research and identify more specific criteria about them like
- identifying the impact on the patient, the caregiver, and the clinical team.
- how much each of them is technologically and regulatory globally and locally feasible.
- identify how much local and global market size and spending.
- not only that but we didn’t forget about adding criteria that reflect how much each one of the team would be excited to work on each of those needs.
Fourth and Final stage
To go from 50 to the top 20 needs and identify the topmost 3 or we call it 1+2) that we should start working on for the next stages. Our approach to making sure that the needs were carefully examined, we did intensive cross research; Each one was doing intensive research for needs that were examined by another member in earlier stages to make sure the results are correct, covered in more depth, and not biased, then reranking took place according to the new inputs.
Now, we know what matters the most and it’s our turn to channel all our power, experience, and knowledge to do something that might relieve some of the pain people are suffering and are willing to do it.
Amr Yousef
Team Bioinformatics, CIF 2020