TEAM GOTHENBURG
A lot has happened since clinical immersion at Alingsås hospital and Lerum commune.
One of our identified needs from the clinical immersion have been on our mind for a while to solve. It causes a lot of suffering for people and expenses for the healthcare organisations around the globe.
Today, let’s talk about urinary catheters.
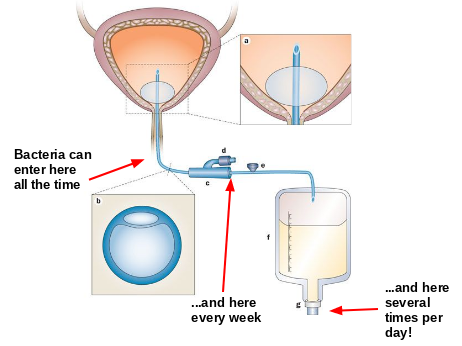
A catheter is a flexible tube that is inserted into a body cavity or channel to remove or add a fluid. A urinary catheter is a tube with one end in the urinary bladder, and is used for draining urine. One of the most commonly used type of catheters are “foley catheters”, or indwelling catheters. Please see the illustrative figure below. A catheter is inserted into the urethra, and kept in place in the bladder with a 10 ml balloon (a) inflated via a port (d). The two holes in the crossectional picture of the tube in figure b are fluid channels for the balloon and the urine. The catheter is connected via a junction (c) to a drainage bag (f) which is strapped to the wearer’s leg. Urine is collected in the bag, and emptied from a drainage port (g) several times per day into a bottle or directly into the toilet.
And no. They are not comfortable to wear.
Why are urinary catheters so important? 15-25% of all hospitalized patients get an indwelling catheter during their stay at the hospital [7]. Some need it because their natural ability to urinate is temporary not functioning properly because of neurological dysfunction (e.g. after a stroke), anesthesia after surgery or because of obstructing scar tissue or tumors, etc. Assuring a proper flow of urine and thus a proper kidney function is vital [8]. From a palliative care perspective, a catheter gives terminally ill people and frail elders a better quality of life through a higher sense of integrity and dignity, when the alternative is to wear an adult diaper or having to struggle going to the bathroom several times per day and night [9].
The biggest issue with urinary catheters are that they get dirty (big surprise!). As time pass, skin and bowel bacteria start to grow a biofilm on the surface of the catheter, spread and cause urinary tract infections (UTI).
[4]
So, what is biofilm? Remember the last time you went to the dentist? And the dentist said: “You should floss. Flossing is good.” And then you said “Yeah , okay. I’ll floss.” And then you went home and flossed your teeth and removed a bunch of white goo from between your teeth. That’s biofilm! Biofilm is basically a shelter made out of secretory products which are released by bacteria to protect them from bactericidal substances like antibiotics and the immune system. It also protects bacteria from naturally being flushed away by urine. Biofilm is a supervillain in a hospital setting, next to multiresistant bacteria. Biofilm grows and spreads on the surface, “ascending” up the catheter to the bladder or urethra and infects the mucous membrane [10].
The risk of getting a urinary tract infection increases with 3% – 7% for each day when you have an indwelling catheter [2][1]. Catheter-associated urinary tract infections (CAUTI) are inevitable after a month of use! CAUTI’s make up more than 30% of all hospital acquired infections [1].
Not only does the infection cause patient suffering with symptoms like fever, chills, abdominal pain and smelly urine, but it takes time and effort to treat for the hospital [11]. What if we could save time from the nurses, doctors, the hospital lab? What if we could shorten the hospital stay with a day or two? [12] What if we could prevent a few of the 13000 annual deaths related to complications of UTI? [2]
Another issue with CAUTI is that the treatment requires antibiotics, which contribute to the global problem of antibiotic resistance [4]. In some countries where use of antibiotics is less regulated, patients with catheter are given antibiotics preventively [5].
Are you convinced yet that CAUTI is worth trying to fix?
Our mission in the past weeks have been looking into ways to prevent bacteria from traveling inside the catheter from the drainage bag to the bladder and cause a symptomatic infection.
We are far from the first to learn that this is a problem, catheter manufacturers and innovators are developing antibacterial catheters. With that in mind, any innovator in this field need to find an edge. You need a specific piece of insight and resource that no one have had before.
There are many different catheters that might reduce incidence of CAUTI. In recent years, antimicrobial technologies have been tested [6]. Why are they not being used instead of the catheters that contribute to CAUTI? You might ask. One problem is the higher cost compared to a non-coated, regular silicone catheter. Another reason is that the doctors and the people who make financial decisions at the hospitals are skeptical about new technologies. There just isn’t enough valid data on the long term effect of the new tech. A third reason might be rigid purchase agreements that hospitals have. Not all hospitals in Sweden have the opportunity to buy silver alloy coated catheters, even though silver coating have shown significant efficacy to reduce formation of biofilm [13].
So, how do we find a solution that meet the needs of all stakeholders around this device? Not only does it have to be simple enough for care staff to actually want to use compared to the benchmark product, but cheap enough to manufacture and bring to the market for hospitals to purchase. It has to be safe enough for the patient to use.
Just like the airplane, the current design of catheters haven’t changed much since the 1930s. It might be a dogma issue. The current solution is well proven. It simply works.
Marcus Bilgec
References
- https://www.who.int/infection-prevention/tools/core-components/CAUTI_student-handbook.pdf
- https://www.cdc.gov/nhsn/PDFs/pscManual/7pscCAUTIcurrent.pdf
- https://www.cdc.gov/infectioncontrol/guidelines/cauti/background.html
- https://www.nature.com/articles/nrurol.2012.68
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4043103/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5316300/
- https://www.cdc.gov/hai/ca_uti/uti.html
- https://alfresco.vgregion.se/alfresco/service/vgr/storage/node/content/25447/Bl%C3%A5sscanning,%20bl%C3%A5stappning%20och%20KAD%20-%20v%C3%A5rdhygien.pdf?a=false&guest=true
- Interview with nurse in palliative team.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3298070/
- https://www.healthline.com/health/catheter-associated-uti#symptoms
- Mail interview with Urologist Henrik Jonsson at Alingsås Lasarett.
- https://www.nursingtimes.net/archive/can-silver-alloy-catheters-reduce-infection-rates-23-07-2011/